How does BFR work?
What is BFR?
Blood Flow Restriction (BFR) is an effective tool for increasing muscle strength, size, endurance, and recovery in both rehabilitation and performance settings (2,4,5). BFR involves using a cuff or tourniquet at the top of a limb (arm or leg) to restrict blood flowing in and out of the limb. When a cuff is placed at the top of a limb, arterial inflow is reduced and venous outflow is significantly occluded, creating a hypoxic, mechanically, and metabolically stressful muscular environment that triggers an increase in proteins and hormones that improve muscle strength, size, endurance and healing (1,4). Usually, it takes heavy loads and high-intensity training to create the muscular environment but BFR creates the muscular environment by combining the restriction of blood flow with light loads and low-intensity training (1,2,4,5).

BFR is a powerful complement to traditional training. It can enhance recovery, help manage fatigue, and provide an effective stimulus when high loads aren’t ideal (2,5). Instead of constantly pushing heavy weights and increasing stress on the body, BFR offers a way to build strength and muscle while minimizing joint strain, muscle damage, and overall neurological fatigue (3,5).
What Happens During BFR?
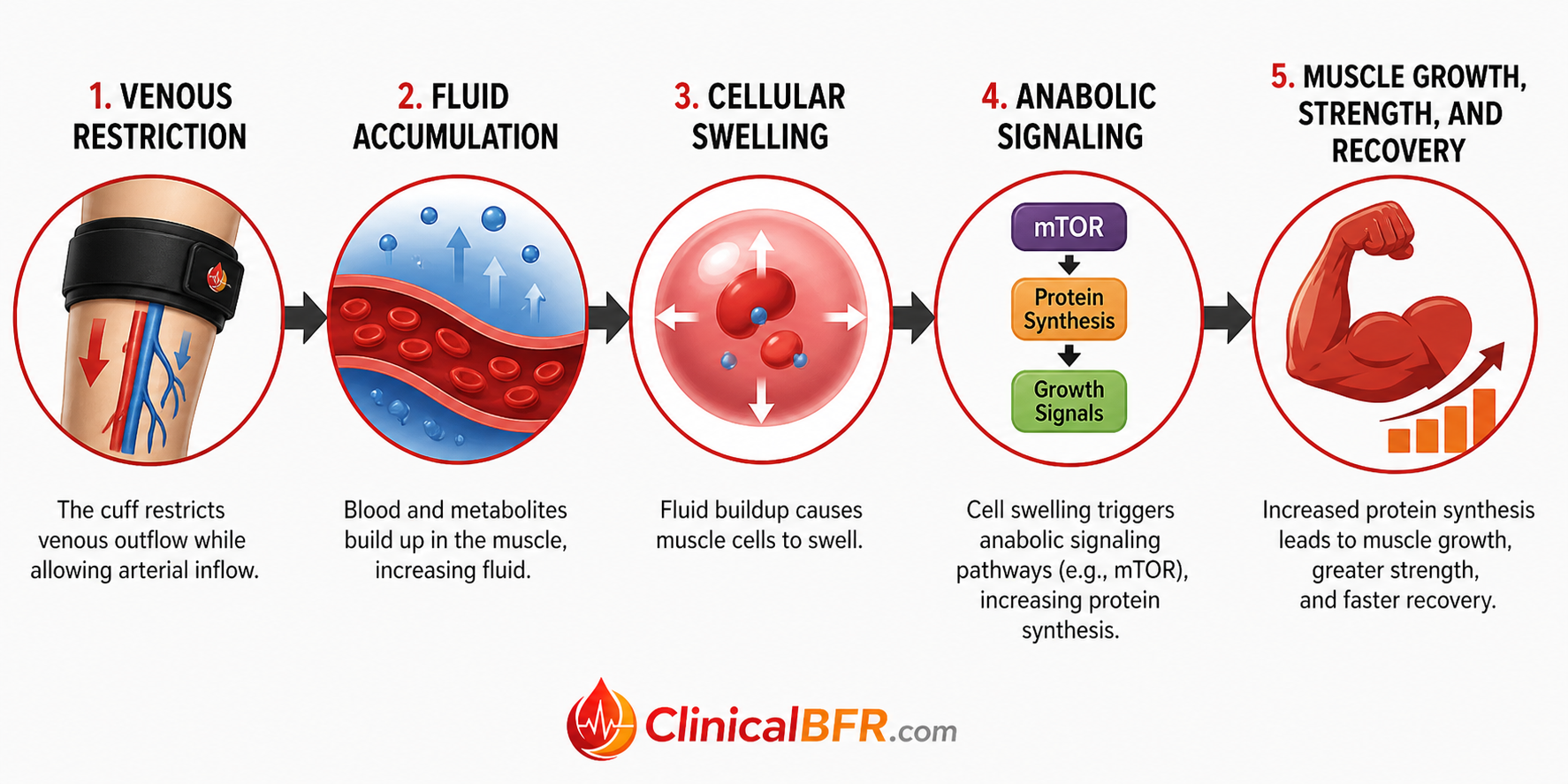
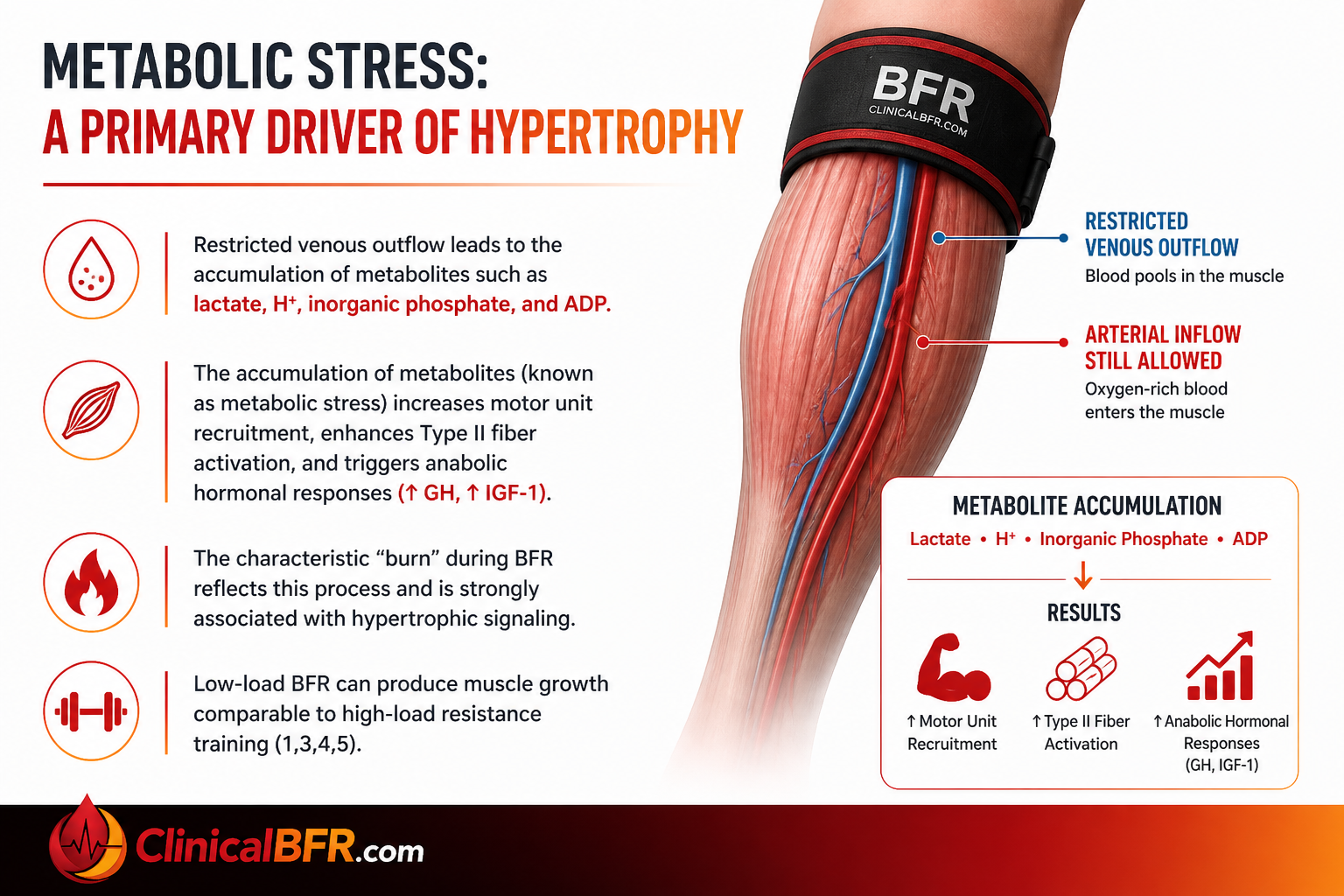
During BFR, a cuff is applied to the proximal portion of a limb, partially restricting arterial inflow while significantly limiting venous outflow. The cuff reduces oxygen delivery to the working muscle, creating a hypoxic environment. At the same time, restricted venous outflow leads to the accumulation of metabolites, producing substantial metabolic stress (2,3,5). A metabolically stressful muscular environment stimulates muscle protein synthesis and promotes the release of key anabolic hormones such as growth hormone, IGF-1, and testosterone (3,5).
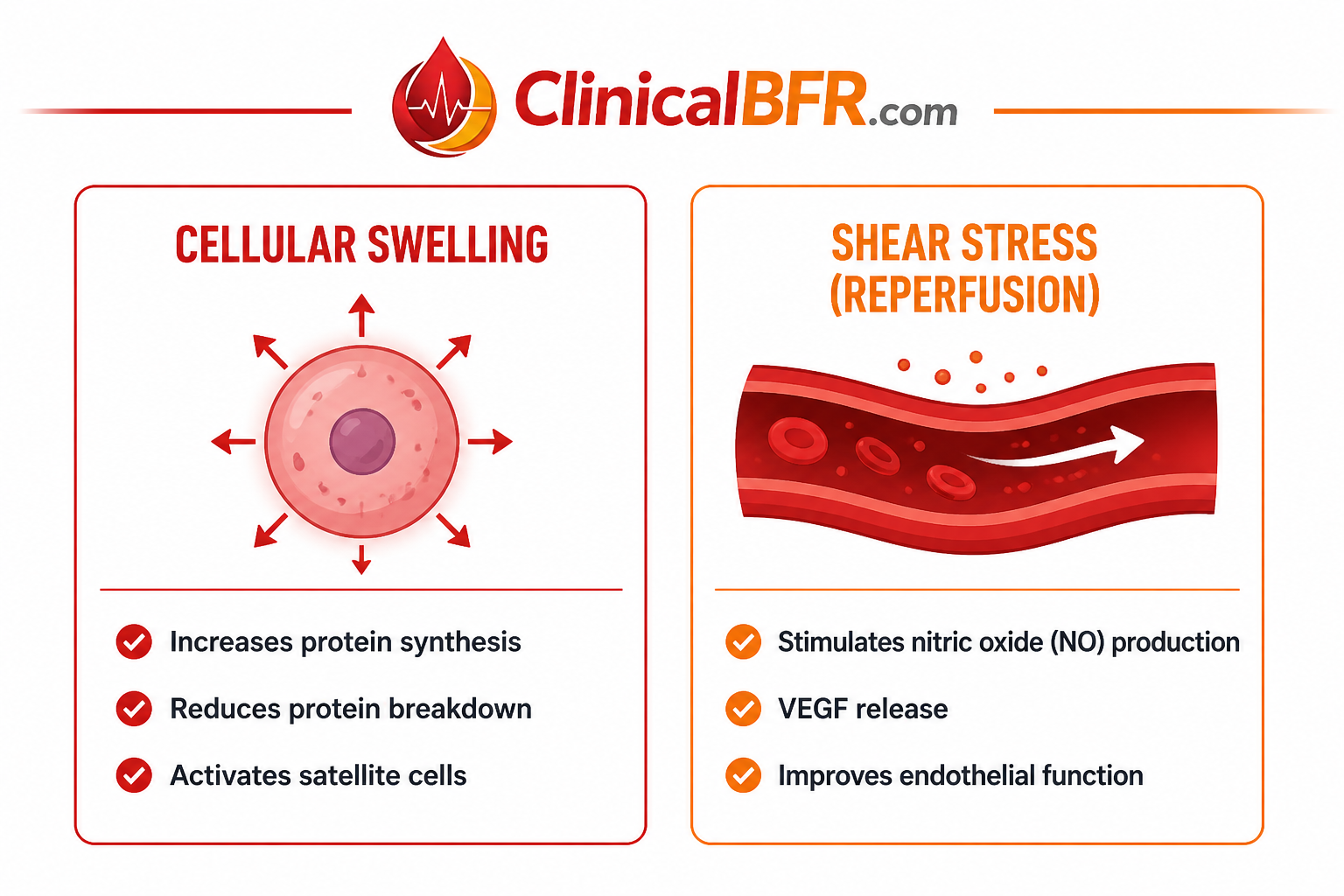
At the same time, BFR generates significant mechanical stress. As venous outflow is restricted, blood pools in the limb, leading to fluid accumulation and cellular swelling. Cellular swelling stretches the muscle cell membrane, activating mTOR signaling, increasing protein synthesis, reducing proteolysis (muscle breakdown), and promoting satellite cell activation for muscle repair and growth. Cellular swelling also enhances the recruitment of Type II fast-twitch muscle fibers even at low loads supporting strength and hypertrophy (1,3,5).
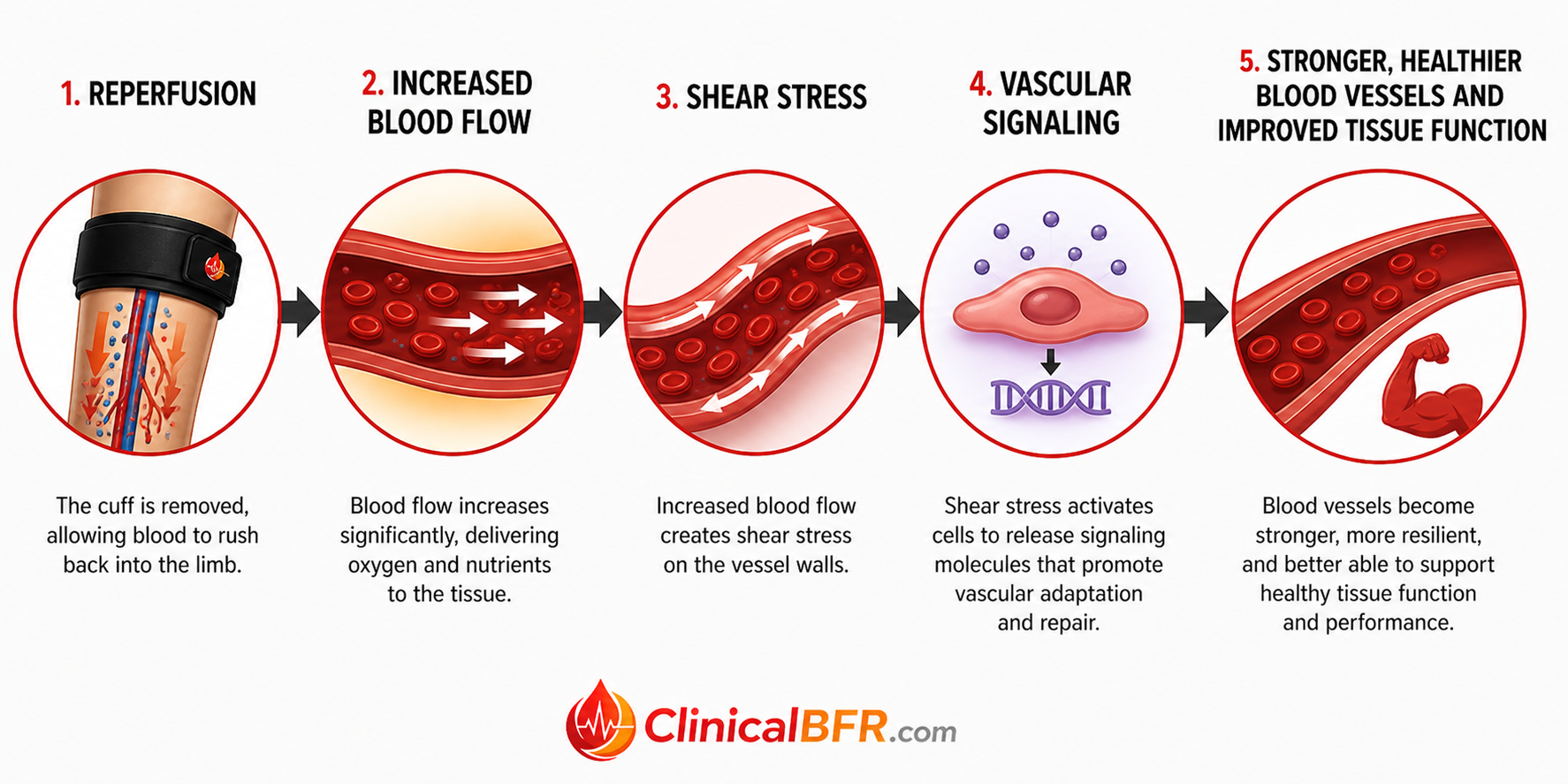
When pressure is released and the cuff is removed, reperfusion allows oxygen-rich blood to rapidly return to the limb. The rush of blood into the limb during reperfusion (rest) creates a shear stress along the blood vessel walls, stimulating the endothelium to release nitric oxide (NO), improving vasodilation and vascular function. Shear stress also upregulates vascular endothelial growth factor (VEGF), promoting angiogenesis (the formation of new blood vessels) and enhancing vascular health (3,5). Over time, this leads to improved circulation, better oxygen and nutrient delivery, and more efficient recovery.
How Does BFR Work?
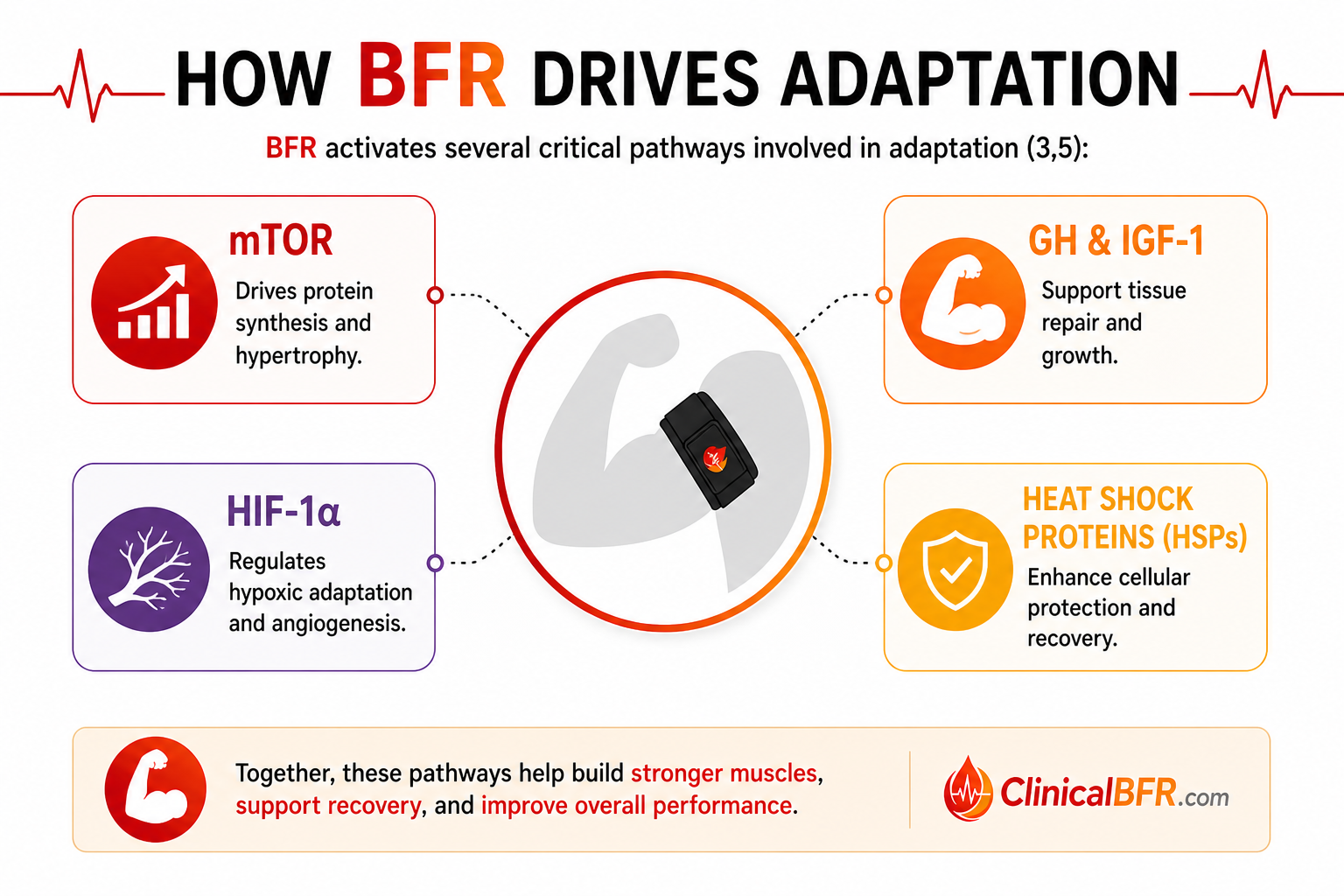
BFR works by creating a muscular environment that closely mimics the conditions created during heavy resistance training. A cuff placed at the top of the limb reduces blood entering the limb (arterial inflow) and prevents blood from escaping the limb (venous outflow) creating a hypoxic (low oxygen) environment, along with significant metabolic stress (accumulation of metabolites like lactate) and mechanical stress (cellular swelling and shear forces) (3,5). In response, the body increases muscle protein synthesis and activates key processes that support cellular function, survival, and adaptation. Together, these mechanisms stimulate powerful molecular pathways including HIF-1α, growth hormone (GH), IGF-1, mTOR, and heat shock proteins (HSPs) which ultimately drive improvements in muscle growth, strength, and recovery.
What three mechanisms make BFR work?
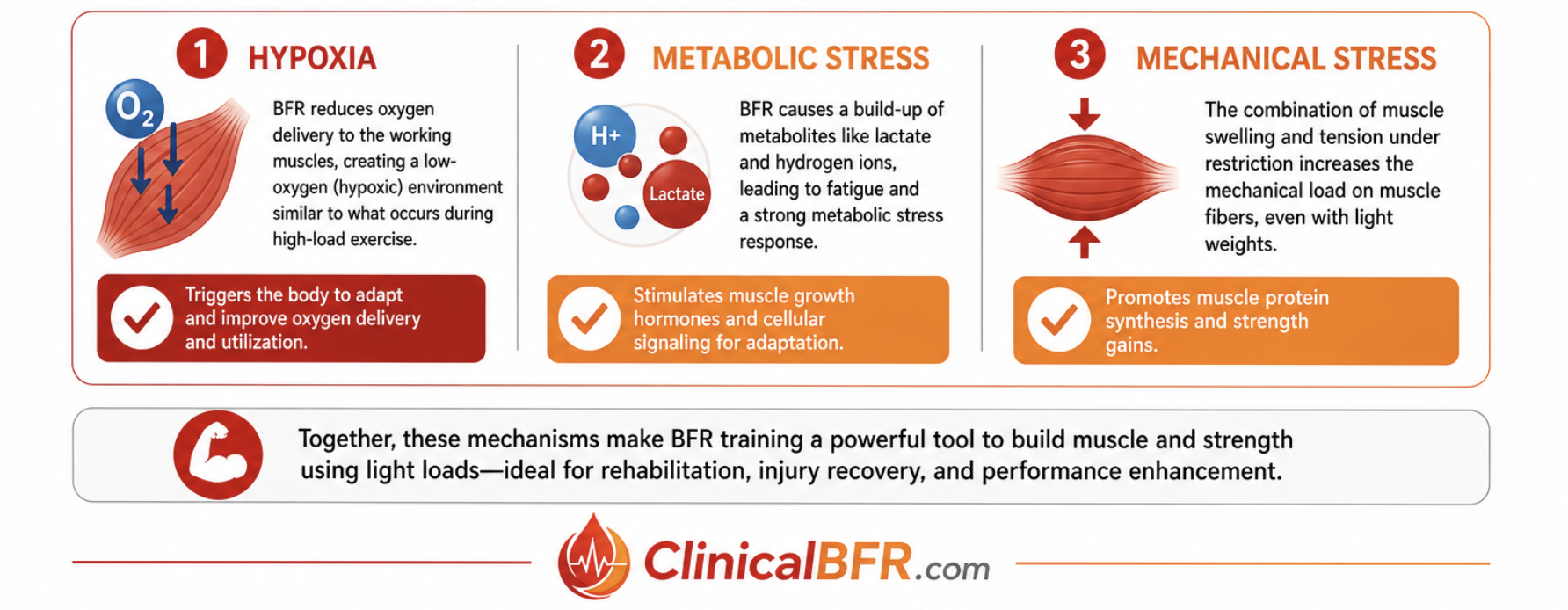
The three mechanisms that deliver the benefits of BFR are hypoxia, metabolic stress, and mechanical stress. The body responds to hypoxia, metabolic stress and mechanical stress by increasing muscle protein synthesis and activating key processes that support cellular function, survival, and adaptation
1. Hypoxia
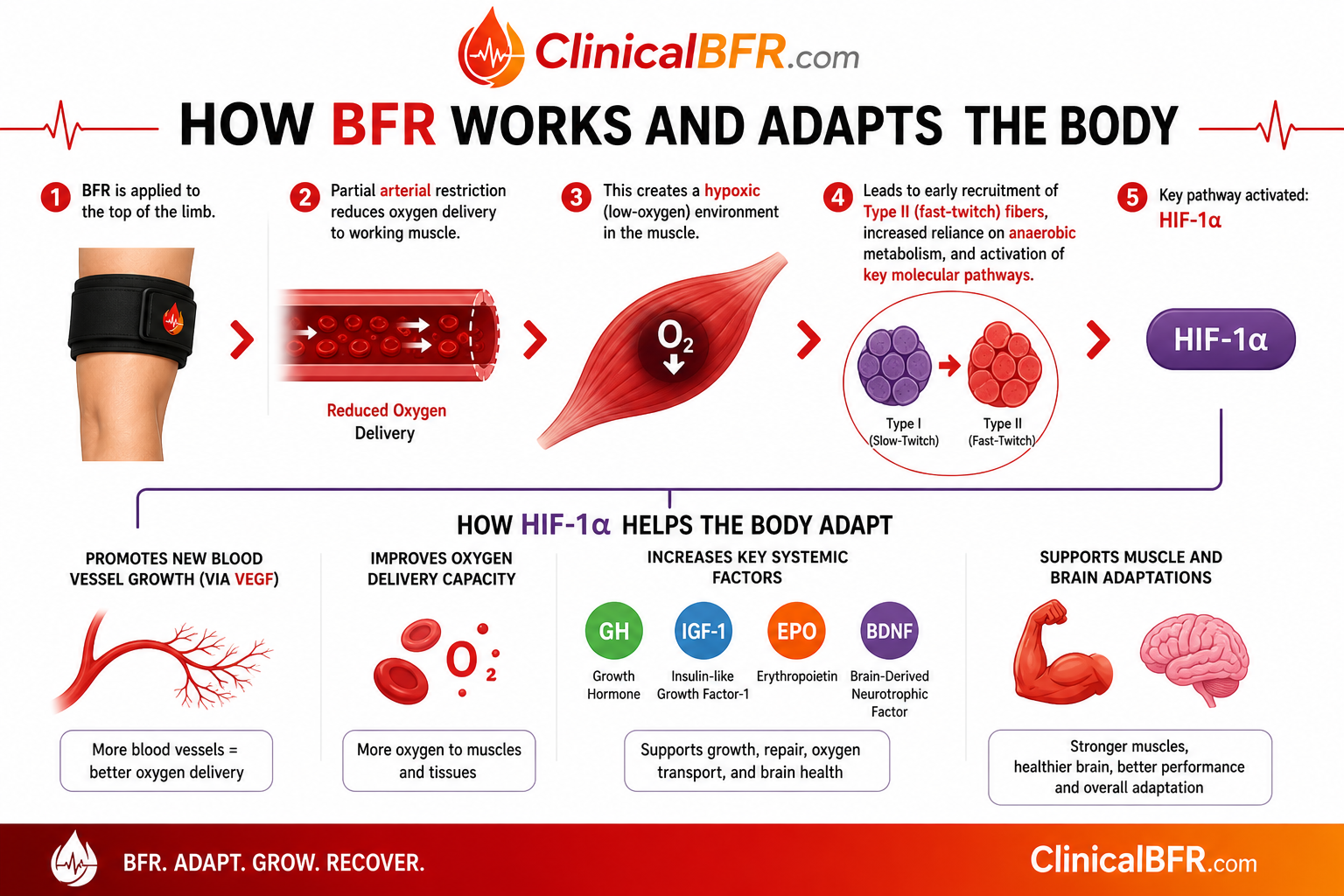
During BFR, partial arterial restriction reduces oxygen delivery to working muscle, creating a hypoxic environment. A low-oxygen muscular environment promotes early recruitment of Type II (fast-twitch) fibers, increases reliance on anaerobic metabolism, and activates key molecular pathways, particularly HIF-1α (2,3,5). HIF-1α helps the body adapt to low oxygen by promoting new blood vessel growth (via VEGF), improving oxygen delivery, and increasing key factors like growth hormone (GH), IGF-1, erythropoietin (EPO), and BDNF, supporting both muscle and brain adaptations.
2. Metabolic Stress
Restricted venous outflow leads to the accumulation of metabolites such as lactate, H⁺, inorganic phosphate, and ADP. The accumulation of metabolites (known as metabolic stress) increases motor unit recruitment, enhances Type II fiber activation, and triggers anabolic hormonal responses (↑ GH, ↑ IGF-1). The characteristic “burn” during BFR reflects this process and is strongly associated with hypertrophic signaling. Low-load BFR can produce muscle growth comparable to high-load resistance training (1,3,4,5).
3. Mechanical Stress
Despite low external loads, BFR creates meaningful mechanical stress through two key processes, cellular swelling and shear stress (3,5). Cellular swelling increases protein synthesis, reduces protein breakdown, and activates satellite cells, all of which contribute to muscle growth and repair. The reperfusion phase, when the cuff is removed following occlusion creates shear stress, which stimulates nitric oxide (NO) production, promotes vascular endothelial growth factor (VEGF) release, and enhances endothelial function. These processes collectively activate key molecular pathways involved in adaptation, including the mTOR pathway for muscle hypertrophy, growth hormone (GH) and insulin-like growth factor-1 (IGF-1) for tissue repair and growth, hypoxia-inducible factor-1 alpha (HIF-1α) for hypoxic adaptation and angiogenesis, and heat shock proteins (HSPs) for cellular protection and recovery.
How does BFR Drive Adaptation?
Why does BFR matter clinically and practically?
Blood Flow Restriction (BFR) matters clinically and practically because it allows clinicians, coaches, athletes, and patients to achieve meaningful strength, hypertrophy, and recovery adaptations using light weights that are far more tolerable for in-season athletes and individuals limited by pain, injury, or post-operative restrictions (1,2). By creating a hypoxic, mechanically stressful, and metabolically stimulating muscular environment, BFR promotes early Type II fiber recruitment, increases anabolic signaling (e.g., mTOR, GH, IGF-1), and enhances vascular and cellular adaptations without the joint stress associated with heavy resistance training (2,3).
Clinically, BFR is a powerful tool to mitigate muscle atrophy, improve strength, reduce pain, and accelerate rehabilitation timelines across a wide range of populations, including post-operative patients, sprains, strains, fractures, and those with chronic conditions.
Practically, BFR provides a scalable, efficient, and versatile training method that can be applied in the gym, at home, or in the clinic, to help individuals create meaningful physiological change with low intensity exercise. BFR helps people “meet themselves where they are” while still driving meaningful physiological change.
References (APA Style)
1. Loenneke, J. P., Wilson, J. M., Marín, P. J., Zourdos, M. C., & Bemben, M. G. (2012). Low intensity blood flow restriction training: A meta-analysis. European Journal of Applied Physiology, 112(5), 1849–1859. https://doi.org/10.1007/s00421-011-2167-x
2. Patterson, S. D., Hughes, L., Head, P., Warmington, S., Brandner, C., & Blood Flow Restriction Exercise Position Stand Group. (2019). Blood flow restriction exercise: Considerations of methodology, application, and safety. Frontiers in Physiology, 10, 533. https://doi.org/10.3389/fphys.2019.00533
3. Pearson, S. J., & Hussain, S. R. (2015). A review on the mechanisms of blood-flow restriction resistance training-induced muscle hypertrophy. Sports Medicine, 45(2), 187–200. https://doi.org/10.1007/s40279-014-0264-9
4. Slysz, J., Stultz, J., & Burr, J. F. (2016). The efficacy of blood flow restricted exercise: A systematic review & meta-analysis. Journal of Science and Medicine in Sport, 19(8), 669–675. https://doi.org/10.1016/j.jsams.2015.09.005
5. Scott, B. R., Loenneke, J. P., Slattery, K. M., & Dascombe, B. J. (2015). Exercise with blood flow restriction: An updated evidence-based approach for enhanced muscular development. Sports Medicine, 45(3), 313–325. https://doi.org/10.1007/s40279-014-0288-1
Frequently Asked Questions About BFR
What are the contraindications of BFR?
Blood Flow Restriction (BFR) training is generally safe when applied appropriately, but there are important contraindications and precautions clinicians should screen for prior to use including, history of stroke, DVT, or clotting issue, severe peripheral vascular disease (PVD), severe hypertension (uncontrolled), compromised arterial circulation / ischemic limb, active infection in limb, recent revascularization or vascular grafting (early phase), pregnancy
What is blood flow restriction (BFR) training?
Blood flow restriction (BFR) training is a method that uses external cuffs to partially restrict arterial inflow and occlude venous outflow during exercise to enhance muscle strength and hypertrophy at low loads (Patterson et al., 2019).
Is BFR training safe?
Yes, when applied with appropriate screening, individualized pressures, and proper supervision, BFR training is considered safe with a low risk of adverse events (Patterson et al., 2019).
How does BFR training work?
BFR training works by creating a hypoxic, metabolically stressful environment that accelerates muscle fatigue and stimulates anabolic signaling pathways similar to high-intensity exercise but with low loads (Pearson & Hussain, 2015).
What are the benefits of blood flow restriction training?
BFR training improves muscle strength, hypertrophy, endurance, and rehabilitation outcomes while using significantly lighter loads than traditional resistance training (Slysz et al., 2016).
What pressure should I use for BFR (LOP)?
BFR pressure should be individualized based on limb occlusion pressure (LOP), typically using 40–80% of LOP to optimize safety and effectiveness (Patterson et al., 2019). It is common for most older adults to start lower than 40% LOP.
Can BFR build muscle with light weights?
Yes, BFR can stimulate muscle hypertrophy and strength gains using low loads (20–30% 1RM) by increasing metabolic stress and motor unit recruitment (Loenneke et al., 2012).
Who should not use BFR training?
BFR training should be avoided or used with caution in individuals with certain conditions such as active clotting disorders, severe cardiovascular disease, previous stroke or DVT, peripheral artery disease (PAD), or uncontrolled hypertension (Patterson et al., 2019).
How often should you do BFR training?
BFR training is typically performed 2–3 times per week, although frequency may vary depending on goals, tolerance, and rehabilitation status (Patterson et al., 2019).
Is BFR good for rehabilitation and injury recovery?
Yes, BFR is effective in rehabilitation because it promotes strength and muscle preservation while minimizing joint stress, making it ideal after injury or surgery (Hughes et al., 2017).
What are the risks or side effects of BFR training?
Common side effects of BFR include temporary discomfort, numbness, or bruising, while serious complications are rare when proper protocols are followed (Patterson et al., 2019).